By David Bautz, PhD
NASDAQ:CVKD
READ THE FULL CVKD RESEARCH REPORT
Business Update
Encouraging Results from Phase 2 HIT Trial
On February 24, 2026, Cadrenal Therapeutics, Inc. (NASDAQ:CVKD) announced encouraging results from the Phase 2 trial of CAD-1005 (formerly CAD-1005) in heparin-induced thrombocytopenia (HIT). The results showed a meaningful reduction in thrombotic events despite not meeting the study’s primary endpoint of platelet count recovery. While platelet recovery did not differ between treatment groups, thrombotic events occurred in 50% of CAD-1005-treated patients compared with >75% in placebo-treated patients, which represents a >25% absolute reduction. Although the study was not powered for statistical significance, the signal is clinically compelling in a condition with a high morbidity and mortality, and no approved therapies specifically targeting the immune mechanism underlying HIT.
The randomized, placebo controlled Phase 2 study evaluated CAD-1005, a selective inhibitor of 12-lipoxygenase (12-LOX) in patients with suspected HIT receiving standard anticoagulant therapy (argatroban or bivalirudin). The trial was initiated by Veralox Therapeutics, which selected platelet count recovery rate as the primary endpoint. The strategic intent of that design was to determine whether platelet count recovery could serve as a surrogate endpoint for clinical outcomes in a future registrational study. In other words, the Phase 2 trial was structured not only to evaluate efficacy, but to test whether platelet count recovery could reliably predict reductions in thrombotic events. Following the acquisition by Cadrenal, the study concluded with 24 randomized patients, 17 of whom had centrally confirmed HIT.
The study did not demonstrate a difference in platelet count recovery between treatment arms. In addition, thrombotic events continued to occur even after platelet count recovery in both arms. This indicates that platelet count recovery may not function as a reliable surrogate marker for clinical efficacy in HIT, particularly in a setting where background event rates remain high despite standard anticoagulation. Rather than representing a setback for CAD-1005, the results help to clarify endpoint strategy. The study successfully answered the scientific question it was designed to address: platelet count recovery does not appear to predict thrombotic outcomes in this context. This now allows Cadrenal to align the development of CAD-1005 around clinically meaningful endpoints, such as thrombotic events.
The key secondary endpoint, incidence of new or worsening thrombotic events, produced the most compelling signal in the dataset, with a >75% thrombotic event rate in placebo treated patients compared to a 50% thrombotic event rate in CAD-1005-treated patients. Although the study was not powered for statistical significance, the magnitude of the reduction in a small, blinded, placebo controlled trial in HIT is noteworthy.
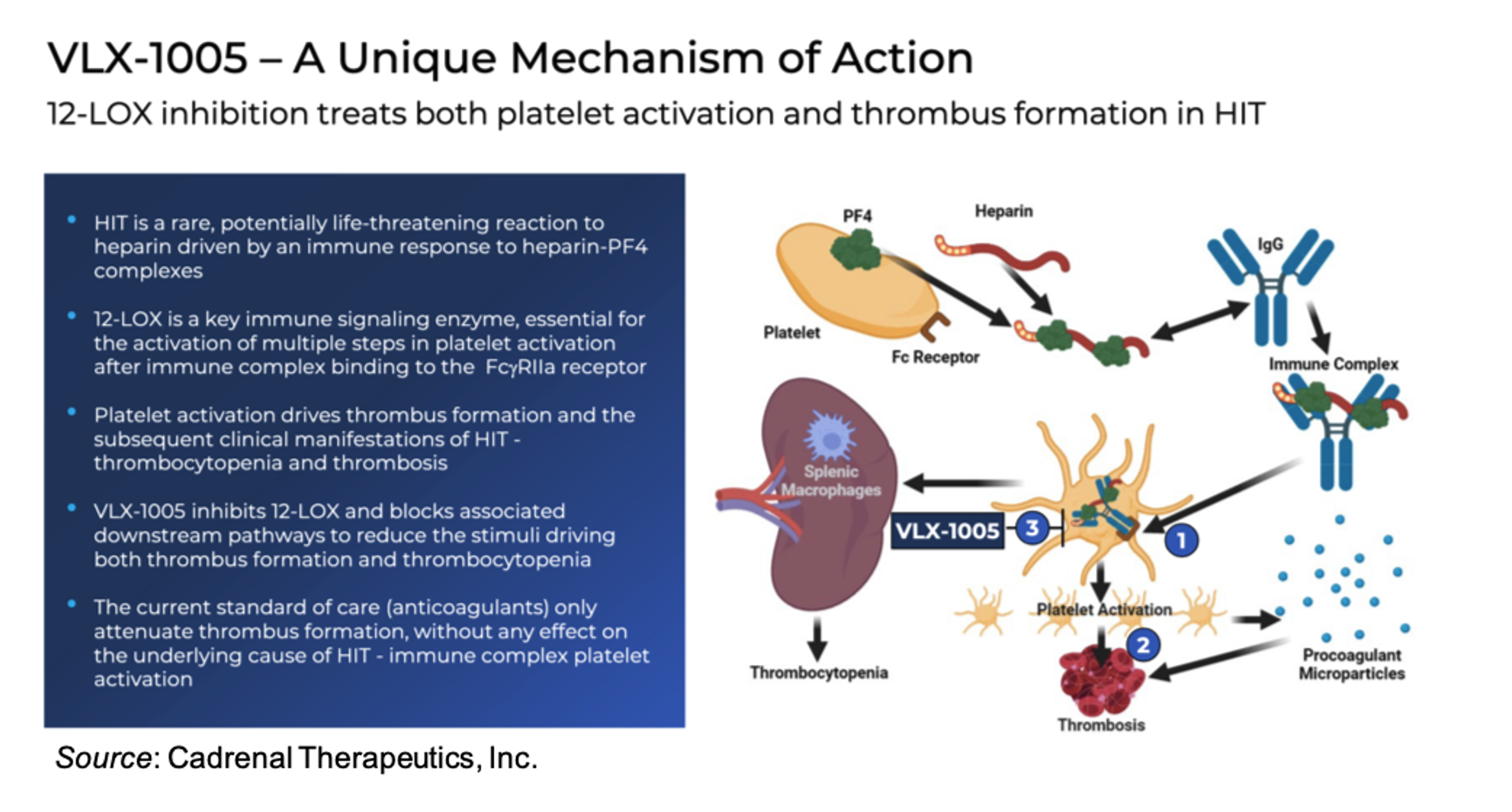
Current management of HIT relies on alternative anticoagulants, which address clot formation but do not target the upstream immune mechanism. CAD-1005’s inhibition of 12-LOX is designed to interrupt the immune signaling cascade responsible for platelet activation on thrombus propagation. The divergence between platelet recovery and thrombotic outcomes in the Phase 2 trial further reinforces the importance of targeting the underlying immune driver (which CAD-1005 does) rather than focusing solely on platelet counts.
Cadrenal has been granted an ‘End-of-Phase 2’ meeting with the U.S. FDA in March 2026 to align with the agency on a Phase 3 registration strategy. The company intends to use thrombotic event reduction as the primary endpoint in Phase 3, build on the safety profile observed to date, and leverage CAD-1005’s Orphan Drug Designation (ODD) and Fast Track status.
Background on HIT
HIT is a severe, immune-mediated prothrombotic disorder triggered by exposure to heparin, an anticoagulant used widely in clinical practice (e.g., surgery, dialysis). It is estimated to occur in approximately 1 in 1500 hospital admissions (Dhakal et al., 2018). Data shows that certain variables can increase the risk of developing HIT, including cardiac surgery (Pishko et al., 2017) and exposure to unfractionated heparin vs. low molecular weight heparin (Warkentin et al., 1995), while a shorter exposure to heparin appears to decrease the risk of developing HIT (Smythe et al., 2007).
Diagnosis of HIT uses the “4Ts Score”, which is a pre-test scoring system that assesses the probability of HIT (Lo et al., 2006). It is calculated as a sum of points from four components: Thrombocytopenia, Timing of platelet count fall, Thrombosis or other sequelae, and oTher causes of thrombocytopenia. Laboratory diagnosis of HIT is divided into two steps: an immunoassay and a functional assay. The immunoassay examines for the presence of anti-platelet factor 4 (PF4)/heparin antibodies. If anti-PF4/heparin antibodies are identified, a functional assay is performed to determine if those antibodies are pathogenic. The 14C-serotonin release assay (SRA) is the “gold standard” functional assay and has both high sensitivity (~0.95) and specificity (~0.95) (Warkentin et al., 2015).
Management for patients suspected of suffering from HIT includes 1) the avoidance of heparin, indefinitely if possible, and 2) use of non-heparin anticoagulation. The duration of non-heparin anticoagulation will be dictated by the presence or absence of thrombosis. Preferred agents for non-heparin anticoagulation therapy include argatroban and bivalirudin, which can be administered IV, or danaparoid, which can be administered subcutaneously.
For patients who develop HIT, there are a number of potential negative outcomes, including thrombosis, bleeding, amputation, increased risk of hospital stay, and even death. Despite decades of research, no approved therapy directly targets the core immune and platelet activation mechanisms in HIT. Current anticoagulants decrease the risk of coagulation but do not modulate immune-mediated platelet activation, which leaves patients at persistent risk of thrombosis.
CAD-1005 for HIT
CAD-1005 is a highly selective inhibitor of human 12-LOX and is designed to reduce or prevent platelet activation and the downstream pro-thrombotic cascade in HIT. By inhibiting 12-LOX activity, CAD-1005 reduces the production of proinflammatory and procoagulant 12-LOX metabolites that feed into platelet activation loops. The drug also addresses the immune-driven aspect of HIT pathogenesis, which is the pathway that links immune complexes and platelet hyperactivity, a mechanism wholly distinct from direct anticoagulation. Lastly, preclinical and Phase 1 clinical trial results indicate there is no increased bleeding signal, which distinguishes CAD-1005 from traditional anticoagulants that reduce the risk of clotting at the cost of an increased risk of bleeding.
12-LOX Biology
12-LOX (encoded by the ALOX12 gene) catalyzes the oxidation of arachidonic acid to proinflammatory lipid mediators such as 12-hydroxyeicosatetraenoic acid (12-HETE) (Dobrian et al., 2011). 12-LOX is expressed in platelets (Contursi et al., 2022), however, unlike cyclooxygenase-1 (COX-1), which drives thromboxane A2 (TXA2) production and classical platelet aggregation, 12-LOX does not primarily initiate aggregation but instead acts as a potentiator and amplifier of platelet activation. The main bioactive product of 12-LOX, 12-HETE, is a lipid molecule that easily transits cell membranes and can induce its effects both intracellularly, where it promotes oxidative stress, and extracellularly, where it impacts a variety of signaling pathways to modulate inflammatory activity. Importantly, 12-HETE does not cause strong platelet activation alone, it just lowers the activation threshold, thus making platelets hyper-responsive (Tamang et al., 2024).
In HIT, platelets are activated via FcγRIIa binding of anti-PF4/heparin antibody complexes (Yeung et al., 2024). 12-LOX acts downstream of FcγRIIa signaling: FcγRIIa activation leads to phospholipase A2 activation that leads to arachidonic acid release. The arachidonic acid is then converted to 12-HETE, and it is the 12-HETE that feeds back to sustain and amplify the activation signal. By inhibiting 12-LOX, pathologic amplification is selectively inhibited by reducing 12-HETE generation. This targets the disease itself and as opposed to current HIT therapies does not result in a residual thrombotic risk. The high selectivity of CAD-1005 helps to preserve baseline platelet function and allows it to be used with standard anticoagulants while being short-lived and controllable in an in-patient setting.
Phase 1 Results
Veralox previously completed a Phase 1a study in healthy volunteers that consisted of a single ascending dose (SAD) and multiple ascending dose (MAD) portion to evaluate the safety, tolerability, pharmacokinetics (PK), and pharmacodynamics (PD) of CAD-1005. In that study, CAD-1005 was found to be well tolerated with no reports of serious adverse events (SAEs), dose-limiting toxicities (DLTs) or discontinuations. The data showed a dose linear increase in key PK metrics with no upper limits on tolerability to the maximum dose tested.
Veralox also completed a Phase 1b drug-drug interaction (DDI) study of CAD-1005 in combination with argatroban, an anticoagulant drug approved for the treatment of HIT. The results showed that co-administration of CAD-1005 with argatroban was well tolerated with no SAEs. Analysis of the PK and PD data showed no evidence for DDI.
Market Opportunity
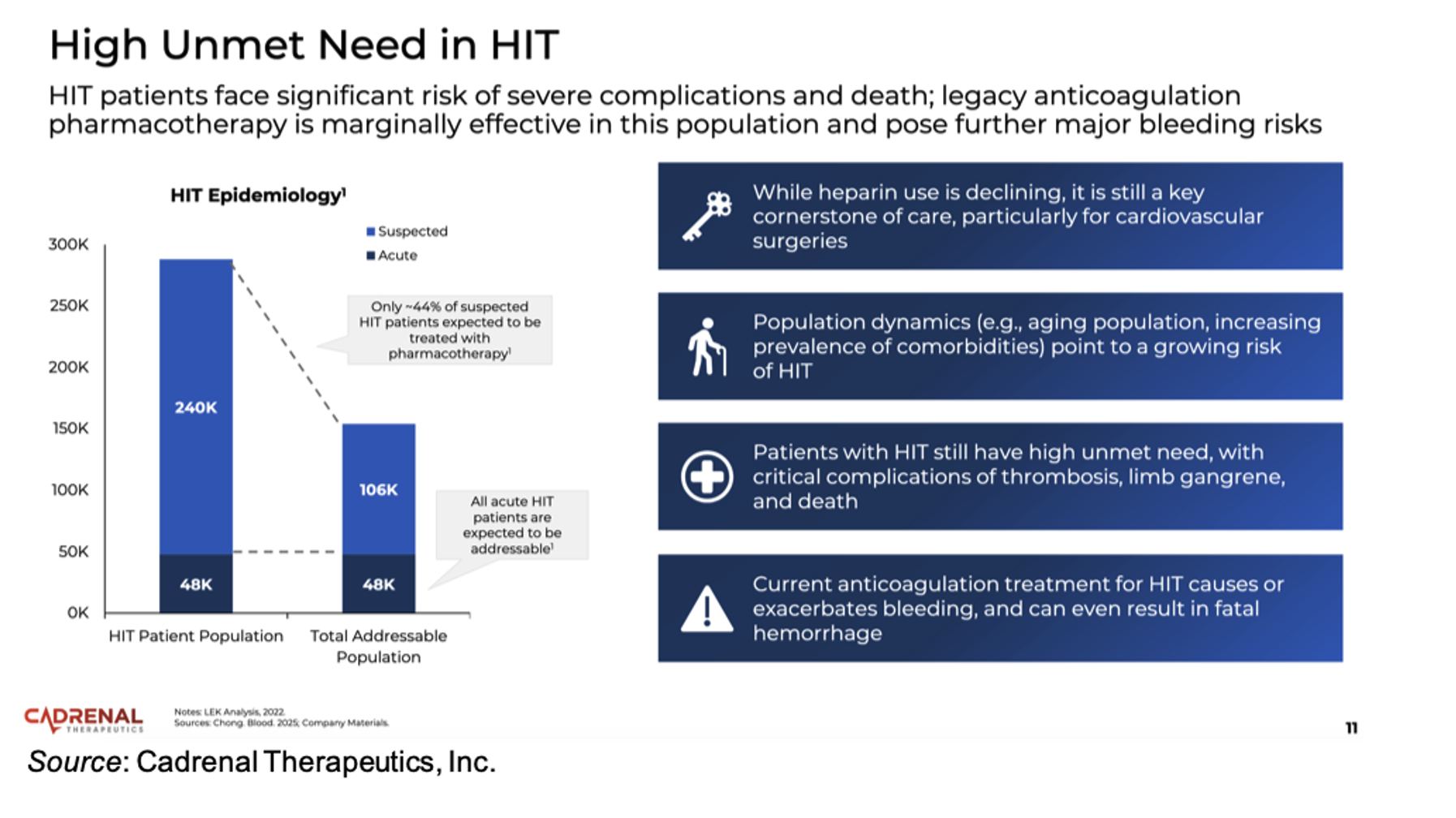
Currently approved HIT treatments focus on non-heparin anticoagulation, which mitigate clot propagation but do not directly modulate immune platelet activation, which is the core driver of HIT pathology. Thus, there is a high residual risk of thrombosis that persists in HIT patients despite anticoagulant therapy. In addition, there are no approved agents that target the immune-mediated platelet activation pathway, thus positioning CAD-1005 as a first-in-class drug. There are approximately 240,000 suspected cases and approximately 48,000 confirmed cases of HIT in the U.S. each year, thus offering a large patient population that could potentially benefit from a safe and effective HIT therapy.
Conclusion
The Phase 2 results for CAD-1005 in HIT were very encouraging as the trial successfully achieved its intended scientific objective (determining if platelet count recovery could be used as a surrogate endpoint) while also revealing a potentially practice-changing signal in thrombotic event reductions. We look forward to the outcome of the upcoming meeting with the FDA as well as additional details regarding the design and timeline for the Phase 3 study. With no changes to our model, our valuation remains at $25 per share.
SUBSCRIBE TO ZACKS SMALL CAP RESEARCH to receive our articles and reports emailed directly to you each morning. Please visit our website for additional information on Zacks SCR.
DISCLOSURE: Zacks SCR has received compensation from the issuer directly, from an investment manager, or from an investor relations consulting firm, engaged by the issuer, for providing research coverage for a period of no less than one year. Research articles, as seen here, are part of the service Zacks SCR provides and Zacks SCR receives payments totaling a maximum fee of up to $50,000 annually for these services provided to or regarding the issuer. Full Disclaimer HERE.