By David Bautz, PhD
NASDAQ: TNXP
READ THE FULL TNXP RESEARCH REPORT
Business Update
Tonmya™ Update
Tonix Pharmaceuticals Holding Corp. (NASDAQ: TNXP) is continuing the commercial launch of Tonmya® following its approval in November 2025. Sales metrics for the first quarter of 2026, which is the first full quarter of sales since the launch, include:
- 2,145 unique healthcare providers prescribed Tonmya
- 3,588 unique patients initiated treatment with Tonmya
- Approximately 5,400 prescriptions were filled, which included bridge prescriptions from the company’s specialty pharmacy channel
Since the launch through April 24, 2026, more than 2,700 unique healthcare providers have prescribed Tonmya, and approximately 5,600 patients have initiated therapy, and through May 1, 2026, more than 11,000 prescriptions have been filled.
The company also continues to make progress on market access. In May 2026, Tonix signed an agreement with a leading group purchasing organization (GPO) providing access to approximately 35 million U.S. commercial lives (~20% of the commercial market). Tonmya is now covered under Medicaid in 38 states, representing approximately 55 million covered lives.
Overall, we view the initial launch metrics as encouraging, particularly given the payer coverage and reimbursement expansion are still in the early stages. First quarter Tonmya net revenue of approximately $3.7 million exceeded our estimate of $2.0 million. However, we continue to maintain a conservative outlook for the remainder of 2026 until prescription trends demonstrate a more sustained and predictable acceleration. While refile and repeat prescriber trends appear positive, weekly prescription growth has remained somewhat uneven thus far, and a portion of early prescriptions were bridge scripts that do not immediately contribute to net revenue. We will continue monitoring for evidence of a cleaner commercial inflection point as payer access broadens throughout 2026.
Update on TNX-4800 – Look at presentation on modeling, it’s in Global Lyme Alliance
Tonix is developing TNX-4800 (formerly 2217LS), a long-acting, human monoclonal antibody (mAb) prophylactic treatment for the prevention of Lyme disease. It is being developed for annual seasonal use in the spring to protect against Lyme disease through the entire tick season in the U.S. There are currently no FDA-approved vaccines or prophylactics to protect against Lyme disease.
In March 2026, Tonix presented Phase 1 data on TNX-4800 at the World Vaccine Congress Washington 2026. The study was designed to evaluate the safety, tolerability, pharmacokinetics (PK), and immunogenicity of TNX-4800 in healthy adults (NCT04863287). A total of 44 subjects were randomized, and 41 completed the study. Each subject received a single subcutaneous administration of placebo (n=10) or TNX-4800 (n=34) at 0.5, 1.5, 5, or 10 mg/kg. TNX-4800 was measurable in the serum at the earliest sampling time of 2-3 days, which indicates rapid systemic absorption. The concentration of TNX-4800 was quantifiable for >200 days in 80% of the subjects in the lowest dose cohort and for up to 350 days in the majority of volunteers at higher doses (≥1.5 mg/kg). The mean half-life ranged from 62-69 days across the different dosing cohorts. The mean exposure to antibody for the 10 mg/kg cohort was <20% of the highest exposures in a rat toxicity study. Anti-drug antibodies (ADAs) were detected in <10% of treated subjects, and the ADAs did not appear to impact PK. The results from this study show that TNX-4800 is generally safe and well tolerated.
Development Plan
Tonix announced plans to initiate an adaptive field study of TNX-4800 in the first half of 2027, pending FDA clearance. It will be a randomized, double blind, placebo controlled, adaptive Phase 2 field study to evaluate the efficacy of a two-dose subcutaneous regiment of TNX-4800 in preventing the first occurrence of confirmed Lyme disease during the primary efficacy surveillance period (Day 3 through Month 6 following administration). Each fixed dose is expected to provide exposures comparable to the 5 mg/kg dose evaluated in the Phase 1 trial. The first dose will be administered in the Spring and the second booster dose will be administered two months later. Eligible participants will be adults and adolescents 16 years of age and older in Lyme-endemic areas in the U.S. The primary endpoint will be the prevention of Lyme disease for six months (comparison of TNX-4800 group and placebo group) from the initial dose.
Tonix will be conducting a Type C meeting with the FDA early in the third quarter of 2026 to discuss the planned Phase 2 field study design. The company is anticipating having GMP investigational product available for clinical testing in time to initiate the trial in 2027.
Background on TNX-4800
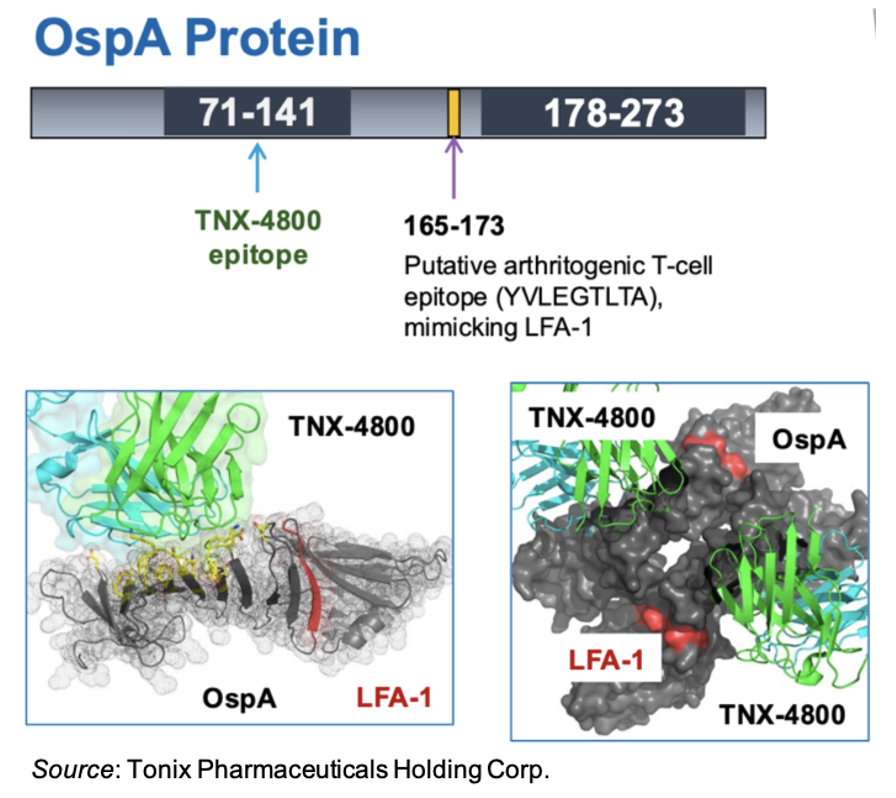
TNX-4800 was developed by researchers at UMass Chan Medical School. It is directed against the outer-surface protein A (OspA) expressed on Borrelia burgdorferi, the bacteria that causes Lyme disease. The OspA protein contains an epitope that mimics human leukocyte function-associated antigen 1 (LFA-1) (Steere et al., 2003). Thus, antibody treatments targeting the OspA protein need to avoid that region in order to decrease the chances for potential autoimmune cross-reactivity. LYMErix™ was an FDA-approved vaccine to prevent Lyme disease, however it was voluntarily pulled from the market due in part to concerns over a possible link to an arthritogenic autoimmune condition that may have been triggered by cross-reactivity to LFA-1 (Nigrovic et al., 2007). Importantly, TNX-4800 does not bind to that same epitope, but instead binds to the 71-141 region of the OspA protein, which has no human homologue.
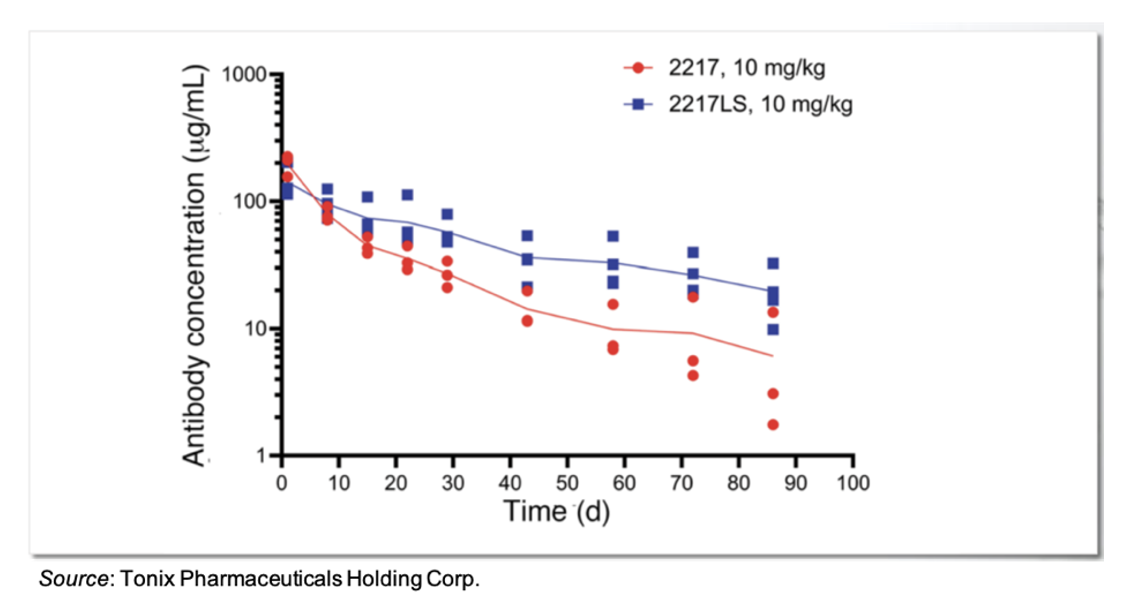
The mAb 2217LS was derived from mAb 2217 by amino acid substitutions to prolong the serum half-life. The following image shows the serum concentration of both mAb 2217 and 2217LS over a 90-day span following injection into nonhuman primates (NHPs).
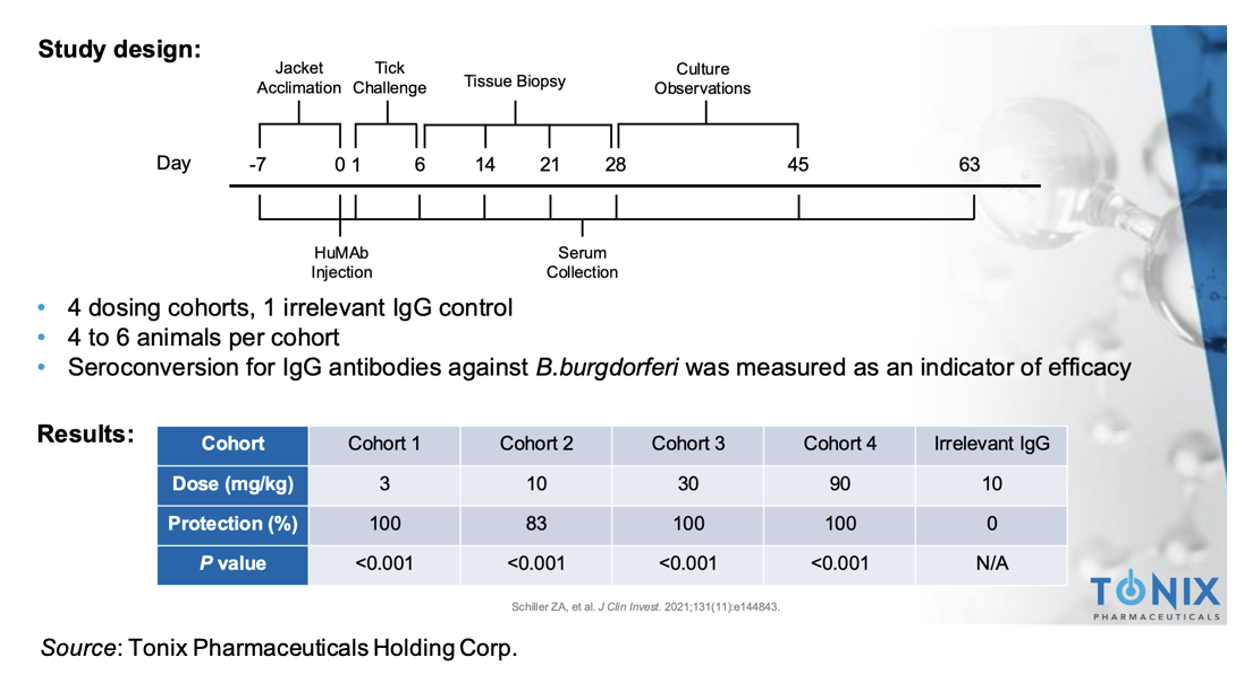
The antibody was tested in an NHP challenge model, in which animals were first dosed with 2217LS before multiple B. burgdorferi-infected ticks were placed on their backs for six days (Schiller et al., 2021). The study included five dosing cohorts: four different doses of 2217LS (3, 10, 30, 90 mg/kg) and a sham IgG (10 mg/kg). The results showed that of the 20 NHPs treated with 2217LS, only one became infected. An overview of the study is given below.
Background on Lyme Disease
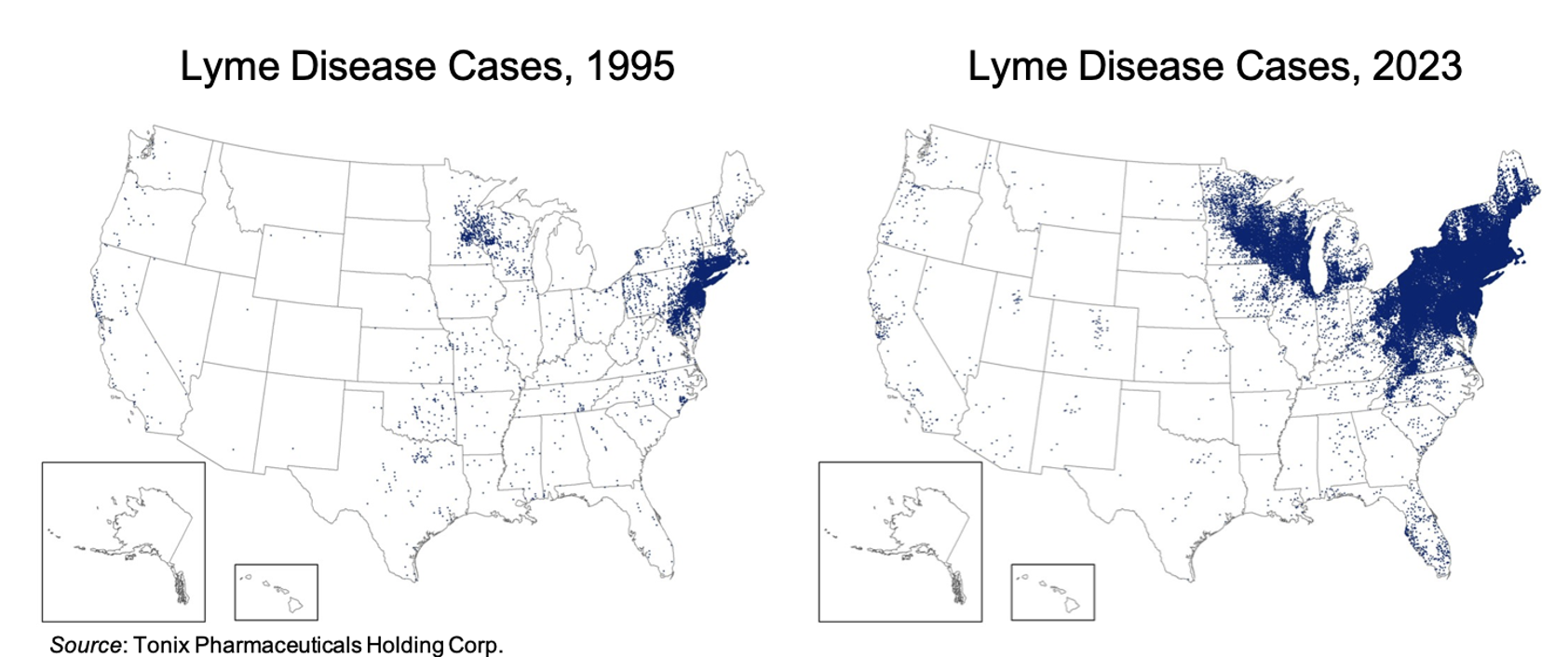
Lyme disease is caused by the bacterium Borrelia burgdorferi. While it can occur all across the U.S., it is reported most often in the Northeast and Midwest. The overall prevalence of Lyme disease has been increasing over time, as shown by the following maps of reported cases from 1995 and 2023 (CDC). There are approximately 80 million individuals in the U.S. that are at risk for Lyme disease.
There are a number of different signs and symptoms for Lyme disease, with the most telling being a rash, which occurs in 70-80% of people (CDC). Additional symptoms of early disease include fever, chills, headache, fatigue, muscle and joint aches, and swollen lymph nodes. Later signs of the disease include severe headaches and neck stiffness, arthritis, intermittent pain in tendons, joints, and bones, heart palpitations, and nerve pain.
B. burgdorferi bacteria live in the mid-gut of ticks and adhere through the outer membrane protein OspA (de Silva et al., 1996). Following a tick bite, iron from the blood of the host down regulates OspA, which causes the bacteria to migrate from the midgut to the salivary glands for transmission (Radolf et al., 2012). While OspA is essential for transmission, it is expressed at very low levels in the human host once transmission has occurred, thus the immune system does not mount an immune response or produce antibodies to OspA. Following administration of an anti-OspA mAb (e.g., TNX-4800), the circulating antibody is ingested by the tick, and it then blocks OspA on B. burgdorferi inside the tick and prevents transmission of the bacteria from the tick to the human host.
Competitive Analysis
Multiple monoclonal antibody preventive treatments have recently been accepted by the FDA and the market. Enflonsia™, Beyfortus®, and Pemgarda™ are monoclonal antibody prophylaxis treatments that have been approved for respiratory syncytial virus (RSV) and COVID-19. Enflonsia, Beyfortus, and Pemgarda are estimated to have 2030 revenues of $955 million, $2.9 billion, and $570 million, respectively (EvaluatePharma). Thus, we view a preventative monoclonal antibody treatment for Lyme disease as a potential blockbuster.
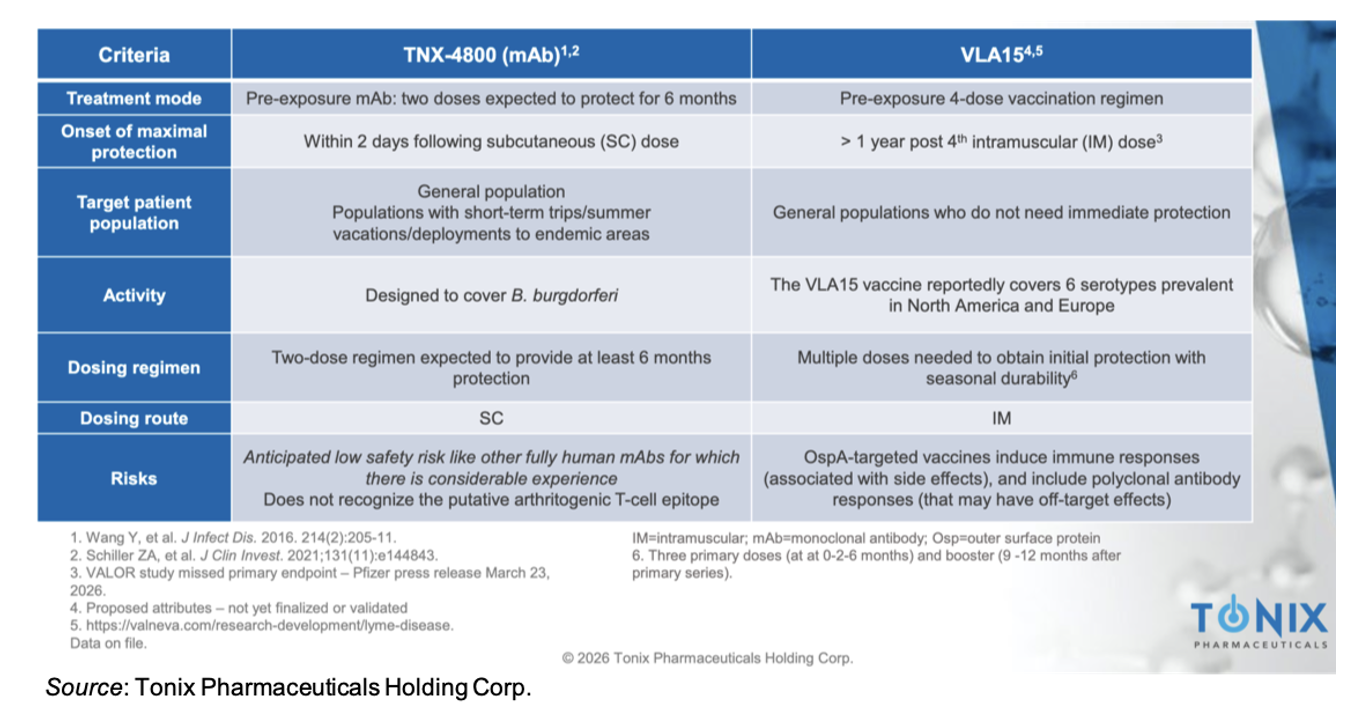
Pfizer is developing VLA15, a vaccine for the prevention of Lyme disease. TNX-4800 has a number of advantages compared to VLA15, which is summarized in the table below. We believe the greatest advantages lie with the rapid onset of protection (~2 days compared to 6-7 months post 3 vaccinations) and only two administrations that provide protection for ≥6 months compared to three administrations needed to obtain protection with uncertain durability.
Phase 2 Study of TNX-102 SL in MDD to Initiate in Mid-2026
In November 2025, Tonix announced that the U.S. FDA cleared the Investigational New Drug (IND) application for the development of TNX-102 SL 5.6 mg for the treatment of major depressive disorder (MDD) in adults. The company is planning to conduct a potentially pivotal Phase 2 trial that will be a six-week, randomized, double blind, placebo controlled study of TNX-102 SL as a first-line monotherapy. Approximately 360 patients will be enrolled across 30 sites in the U.S. The primary endpoint of the study will be the MADRS total score change from baseline at Week 6, with secondary endpoints that include global impression scores, anxiety ratings, and measures of sleep disturbance and sleep quality. Startup activities have begun, and we expect the trial to initiate enrollment in mid-2026.
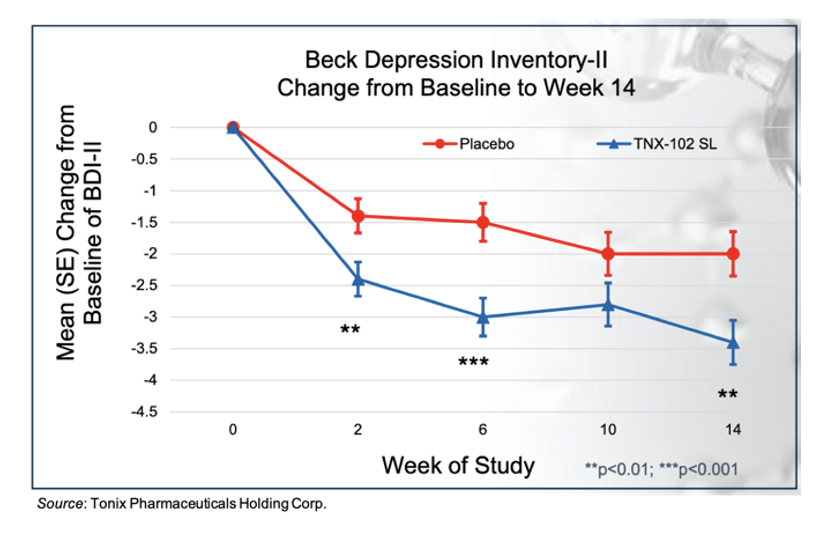
The support for evaluating TNX-102 SL as a treatment for depression stems from results of TNX-102 SL in fibromyalgia and post-traumatic stress disorder (PTSD) clinical trials. For example, in the RESILIENT Phase 3 trial, there was a greater reduction in the total Beck Depression Inventory-II score in the TNX-102 SL cohort compared to placebo at Week 14 with an effect size of 0.27, as shown in the following figure.
Financial Update
On May 11, 2026, Tonix announced financial results for the first quarter of 2026. Net product revenues for the first quarter of 2026 were approximately $6.9 million compared to $2.4 million for the first quarter of 2025. Net revenue from sales of Tonmya for the first quarter was approximately $3.7 million. Cost of sales in the first quarter of 2026 was approximately $1.6 million compared to $0.9 million for the same time period in 2025.
R&D expenses for the first quarter of 2026 were $18.2 million, compared to $7.4 million for the first quarter of 2025. The increase was primarily due to pipeline prioritization and increased headcount. G&A expenses for the first quarter of 2026 were $28.6 million, compared to $10.1 million for the first quarter of 2025. The increase was primarily due to spending on sales and marketing related to Tonmya along with increased headcount.
As of March 31, 2026, Tonix had approximately $185.5 million in cash and cash equivalents. Subsequent to the end of the quarter, the company raised approximately $22.6 million in proceeds utilizing its at-the-market (ATM) facility. We estimate that the company’s current cash position will finance operations into the second quarter of 2027 but not beyond. As of May 8, 2026, Tonix had approximately 15.9 million shares outstanding and, when factoring in stock options and warrants, a fully diluted share count of 17.7 million.
Conclusion
We view the initial commercial launch of Tonmya as encouraging, with early prescribing trends and first quarter revenue exceeding our expectations. Net revenue of $1.4 million in 4Q25 and $3.7 million in 1Q26 came in ahead of our prior estimates, reflecting early physician adoption following the product’s November 2025 approval. While initial prescriber uptake has been favorable, we continue to maintain a measured outlook for the remainder of 2026 until prescription growth demonstrates a more sustained and predictable acceleration. We currently project 2026 Tonmya net revenue of $18.9 million and expect continued progress in payer access and physician awareness to support ongoing commercialization efforts. In addition to Tonmya, we expect details regarding the company’s Type C meeting with the FDA in the third quarter of 2026 as it finalizes designs for a field study of TNX-4800 in 2027. With no changes to our model, our valuation remains at $64 per share.
SUBSCRIBE TO ZACKS SMALL CAP RESEARCH to receive our articles and reports emailed directly to you each morning. Please visit our website for additional information on Zacks SCR.
DISCLOSURE: Zacks SCR has received compensation from the issuer directly, from an investment manager, or from an investor relations consulting firm, engaged by the issuer, for providing research coverage for a period of no less than one year. Research articles, as seen here, are part of the service Zacks SCR provides and Zacks SCR receives payments totaling a maximum fee of up to $50,000 annually for these services provided to or regarding the issuer. Full Disclaimer HERE.